 Eons have passed since our last informational entry which is an eternity in the blogosphere. As a high school teacher I am at last on summer vacation with some time on my hands to return to this place we have put together to encourage others to research and evaluate their lifestyles and make healthy, educated choices.
I have been told that it is madness to move during a school year as a teacher. Well, Tim and I purchased a home and moved at the end of February. Life is wonderful! Or at least it should be considering we now have a place to do as we want to with gardening and hosting international friends. Two weeks prior to our move Tim was hit by a car while riding his bike through a parking lot at a bike race. The driver simply did not look before backing up in the crowded lot. Needless to say, his RIGHT hand was dislocated and broken and surgery ensued a week before our move. Eight weeks later the 3 pins came out and at ten weeks his cast came off. He's been in rehab to get his hand fully functional again and we are still mopping up all the medical bills and his bicycle replacement, etc. So, thus, the reason we have not posted sooner. On the bright side, we love our home and things are returning to normal. We are back on the road again... This month, I left the mid forties for the late forties, and I love it! My focus for this entry is about listening to your body by actively thinking about why you might feel the way you feel or why you are encountering symptoms you might be encountering. Now that Tim and I have been in nutritional ketosis for 11 months, here are some things that have transpired in my own learning about managing this state of life. In our last info blog Tim wrote about niacin. We both stopped taking it every day after we started getting phantom flushes. Phantom flushes are flushes that felt the same as a niacin flush but we had not taken any in hours. Tim used it again to detox off pain medication after surgery and it is a great supplement for various other detoxification needs. One of the biggest things that I have noticed is that my weight has become very stable. It is so stable that I now wonder if this is just where I'm going to be the rest of my life. In my life I've never had the luxury of weighing the same day after day, it has always shifted by pounds. This has completely stopped! I'm sitting at 143 ish and I am usually up or down within a pound. I reached a point in March where I was not feeling really wonderful anymore and decided to try some changes. I started adding more carbohydrates back into my diet based on feelings. I know, no emotional eating. I'm talking about physical feelings. I was having a hard time with recovery after riding. I began to notice that it took about 3-4 days for me to recover instead of feeling great the next day after my 40+ mile rides. I learned to recognize when my glycogen stores were low and this lead me to eat raisins or a slice of toast immediately after a longer ride. Now I can do those longer rides and feel ready to ride again the next day, but it seems to take a slice of toast or dried fruit to get my glycogen stores back to full. If I had a performance study done I would know where to keep my heart rate in order not to tap those stores and only burn fat. Tim can thrive on half the amount of carbs that I seem to require. Listening to your body is absolutely essential! There is a blood test I am thinking about that helps you find your optimal carb level which can range from 25 grams to 100 grams per day. I am feeling great again at about 75-80 grams per day and my weight is the same, which I know from experience, if the additional carbs were a bad idea, I'd be going up with my weight. Another reason for me to increase my carbs is that some of the things that I have done to manage other areas of my life needed to return. This last spring my allergies were very terrible, some of the worst I have experienced in my life. I decided to bring back the yogurt and local honey which control allergies for me and I've had no more problems. This means 9 grams of carbs from yogurt and 10 grams from the teaspoon of honey, but I feel great and I'm not taking allergy drugs, plus my weight is the same. I need to update my "what I eat" page. After taking a nutrition class this last semester I learned that I need more variety, so I'm working on that over this summer. Of course my diet was "bad" for my class assignment which made it easy for me to complete the assignment created for self-evaluation of your own nutrition. I also learned a great deal on sanitation and keeping the kitchen sanitized, another area to up my game in. Stay posted, we are going to be working on catching up here. In previous musings here, I wondered if having more fats in the body (not on the body) circulating through the skin was giving us sun protection because we noticed that we were suddenly getting sunburned less shortly after switching to high fats in our diets. You can see the initial results in our 3 month picture. To our surprise, there was an article published about this very thing! Here's the link to the article: http://www.foodrenegade.com/should-you-use-sunscreen/ . In my photo pictured here you will notice my funny tan lines. Well, tested out what my sun endurance is now by riding in the late morning to early afternoon for 2 to 2.5 hours without any sunscreen just to see how long it would take for me to burn. I had a slight burn at the 3 hour mark! Thus my funny tan lines. This is simply amazing because before changing our diets I would have the same pink in 20-30 minutes! My additional musing about Vitamin D is in the works for my next blood test. I have had tremendous trouble getting my Vitamin D levels in the normal range for several years. Vitamin D deficiency leads to osteoporosis which runs in my family and every case was preceded by chronic low Vitamin D. I live in a very sunny place and people all over my city, myself included, have low Vitamin D. Stay posted for those results along with my other blood numbers. Hopefully by now you understand that a lifestyle of nutritional ketosis is very individualized and its essential that each person learns to listen to their own body. The photograph above was taken of me today, 11 months of this lifestyle, I'm sure you can see the difference for yourself between me at the beginning, at 3 months, to now. I weigh the same as I did at 3 months in but I'm so much smaller. I'm stronger and faster on my bike (remember you can follow us on Strava.com, it's free). Here's wishing you a healthy and vibrant summer stay tuned in... Lynette
0 Comments
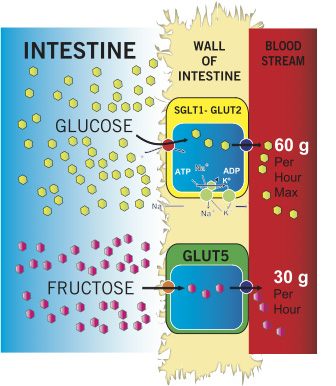
 Renowned neurologist David Perlmutter, MD, blows the lid off a topic that’s been buried in medical literature for far too long: carbs are destroying your brain. And not just unhealthy carbs, but even healthy ones like whole grains can cause dementia, ADHD, anxiety, chronic headaches, depression, and much more. Dr. Perlmutter explains what happens when the brain encounters common ingredients in your daily bread and fruit bowls, why your brain thrives on fat and cholesterol, and how you can spur the growth of new brain cells at any age. He offers an in-depth look at how we can take control of our “smart genes” through specific dietary choices and lifestyle habits, demonstrating how to remedy our most feared maladies without drugs. In Grain Brain, Dr. Perlmutter offers suggestions on how to fuel the brain properly with sound nutrition. These basic changes can help alleviate, or even reverse brain disease, eliminate brain fog symptoms, and improve memory and energy levels. Check out this short video for more info. It is so refreshing to read a book by a brilliant man who has done the research that aligns with our lifestyle. He is really onto something significant. He has clinical research to support his claims that carbs are killing us as a society. It's a NT Times best seller, #1 right now. Dr. Perlmutter is very vocal about the destructive effects of grains and carbs on our brain. The frequency of mental disorders like, depression, ADHD, alzheimer's and other cognitive issues. also  It seems the topic of calories comes up all the time. Everyone thinks that counting calories will cause weight loss. If you burn more than you take in, you'll lose weight. 3,500 Kcal = 1lb of fat, right? After all, you cannot argue with the first law of thermodynamics, right? Which basically states that you cannot destroy energy, conservation of energy is the law. Yes that is true, but maybe we need to have a quick physics lesson. The law states, "The law of conservation of energy states that the total energy of an isolated system is constant" So, is your body an isolated system? (See picture to the left) No, it is not. Also, is your body 100% efficient in turning your food energy into fuel? No, it is not. If your body does not use the fuel it goes out in the form of waste or is stored as fat. So the question is, what kind of calories are you consuming? Here is an extreme example: Take 1 cup of olive oil and drink it. You'll be getting about 1920 Kcal worth of energy in the 224 grams of fats, 0g carbs. What will happen? Provided you don't vomit, most people know what will happen. You'll get diarrhea, why is that? Your body cannot use all of those calories with perfect efficiency so it dumps any excess. So our body is not an isolated system. Fat uptake is regulated by the pressure gradients and absorbed by the lymphatic system. So if your lipid levels are full, your intestines will let it pass. See Fig.1 Now, let's talk about carbs. These behave much differently because it uses a different metabolic system to harness the energy. If you were to drink 8 20oz bottles of cherry Coke, you'd have 2080 Kcal's via 560g of sugars. Provided you don't vomit or go into shock, what happens to these calories? Your body only needs 5g of sugar in your bloodstream at one time, anything above that destroys tissue. So your pancreas comes to the rescue and pushes the extra 555g of sugar into your fat stores with a rush of insulin. See fig. 2
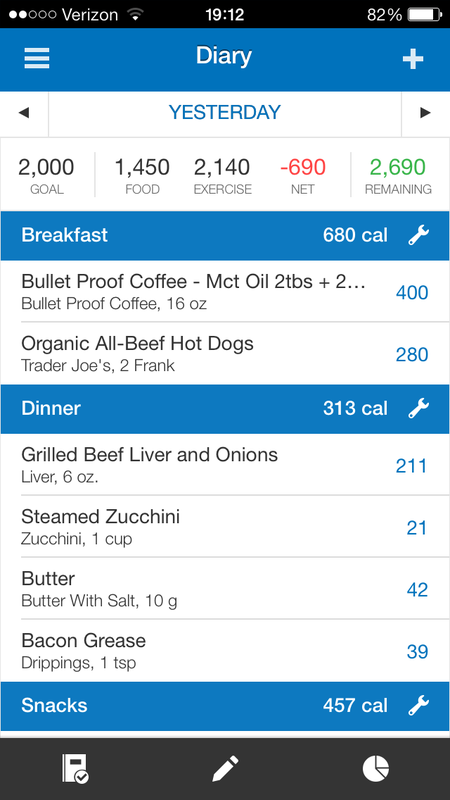
So if your body gets a large dose of calories, it really depends on what kind they are. Generally speaking, carbs are digested quickly and turned to fuel then deposited into the bloodstream, depending on work being performed are converted into ATP with CO2 as a byproduct. The remaining glucose is transported into adipose tissue (body fat). Fats are processed differently all together and enter the bloodstream as triglycerides where they are available for muscles to use for fuel as ATP. Any remaining fats that are not needed will not be stored, but eliminated via waste. 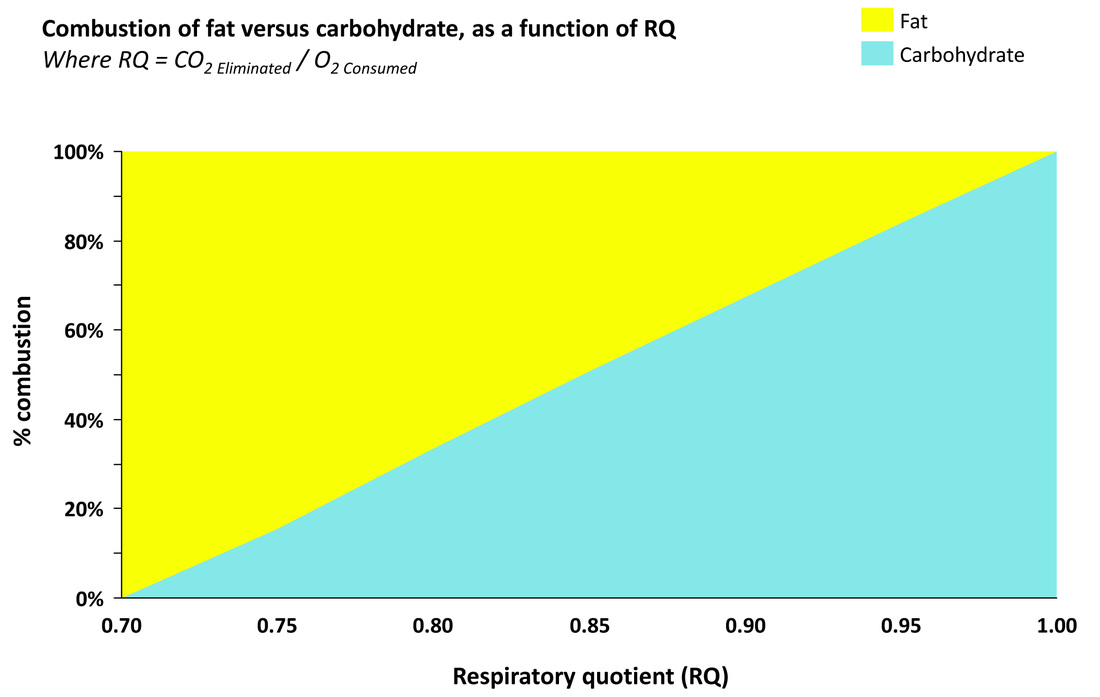 Fig. 3 Fig. 3 Calories Out All exercise is not created equal. Sprinters use the creatine cycle, they don't tap fats or glycogen stored in the muscles and liver. Middle distance runners who are 2 through 120 minute efforts like 800m to 15,000m are tapping into glycogen stores almost exclusively. Fig. 3 shows how your body uses the two main fuel systems as you work harder in your workouts. It's pretty fun to see this in action, when you're burning carbs, you produce more CO2, thus you have to breathe harder to eliminate the CO2 from your body. But when you're oxidizing fat, you produce quite a bit less CO2 and can improve your performance with less panting. You also don't feel the burn as quickly into a long steep climb as you would if you're burning carbs for fuel. There is a great article by Dr. Peter Attia on his journey to ketosis as measured in his performance. He proves pretty clearly that ketosis is a much better system for the endurance athlete. I do not count calories to manage my weight, it seems to make no difference at all. Dr. Steve Phinney has been living in nutritional ketosis for 30 years, his weight has been stable during that time however, his calories can fluctuate from 2,000-6,000 per day. Here is an example from MyFitnessPal app. It's great except for the assumption that my body is 100% efficient. Also, my lean body mass happens to be 137 lbs. So there might be a little something wrong with their calculation.
Here are a few links to articles & studies about how the ci/co theory does not work.
Dieting does not work UCLA Reality trumps myth Nova article
As I have been researching ways to improve my lipid profile, I started reading a bunch of research on Niacin (vitamin B-3). It comes in a few forms, some good, some not so much. The benefits are flat-out amazing! Niacin, also known as nicotinic acid and vitamin B3, is a water soluble, essential B vitamin which when given in high doses is effective in lowering low-density lipoprotein (LDL) cholesterol and raising high density lipoprotein (HDL) cholesterol. Which is better than statin drugs that lower all cholesterol, including the good stuff. There are 3 main forms of niacin, nicotinic acid, niacinamide and inositol hexanicotinate. The later is the extended release or sustained release that is not very safe. Niacinamide is the most common form because it does not trigger the flushing response, but is less effective for certain conditions. The best part is that niacin is cheap and pharmaceutical companies cannot patent it.
I want to do a fair and balanced report here, so I will do my best to show both sides, but frankly, I like niacin, in fact, I'm doing a niacin flush right now, my skin is starting to get red and warmer as I type. So let's start with a recent study that headlines, "Niacin Therapy Shows No Benefits, Has Some Harmful Effects" it opens with this, "Mar. 11, 2013 — A highly anticipated study evaluating a combination of the vitamin niacin with the anti-flushing agent laropiprant finds the therapy provides no benefit to and may even be harmful for patients with vascular disease, according to research presented today at the American College of Cardiology's 62nd Annual Scientific Session. Detailed trial data is presented here for the first time." Now, here comes the study, (I hope this serves as a lesson on how to read studies, because this one has some serious inconsistencies.) They did a good job at selection and randomization with placebo. See if you can spot the issues in isolating niacin's impact. Click the link to see an article that highlights the study details. "The four-year study tested a combination of extended-release (ER) niacin with laropiprant in patients at risk for cardiovascular problems such as heart disease and stroke. The 25,673 patients in the study were randomized to receive ER niacin/laropiprant 2g/40mg or a placebo, and all received commonly prescribed LDL cholesterol-lowering medication simvastatin (with or without ezetimibe)." OK, I hope you got this quiz right. They were all on statin drugs, they chose the extended release and had laropiprant to reduce the flushing effect that normally occurs with niacin. Let's take a look at their findings that they published for the world to see. "The study did not meet the primary endpoint of reducing the chances of a major vascular event, defined as the composite of non-fatal heart attack or heart-related death, stroke, or need for angioplasty or bypass surgery. Patients receiving ER niacin/laropiprant had a similar number of major vascular events as patients receiving placebo (13.2 vs. 13.7 percent, p=0.29). The study also found unexpected and significant excesses of bleeding (2.5 vs. 1.9 percent) and infections (8.0 vs. 6.6 percent) among the ER niacin/laropiprant patients. In addition, significantly higher numbers of patients receiving the study drug suffered serious known side effects including new onset diabetes (9.1 vs. 7.3 percent), diabetic complications (11.1 vs. 7.5 percent), gastrointestinal problems such as indigestion and diarrhea (4.8 vs. 3.8 percent), and skin issues including itching and rashes (0.7 vs. 0.4 percent)." First, using extended release niacin has been proven to produce unacceptable side effects, primarily liver damage. "Significant hepatotoxicity is particularly common with high doses of sustained release niacin. In many cases, the injury becomes apparent after a dose increase or after switching from the regular crystalline to a sustained-release form." Second, laropiprant has been recalled, "Merck & Co has said it is recalling Tredaptive cholesterol tablets in response to trial results that raised safety concerns and the recommendations of a European Medicines Agency safety panel." The US regulators rejected laropiprant for market release in 2008. So, why would you continue a study with a product that was rejected by the FDA? Third, why were the subjects all on statin drugs? It seems that there are too many chemical interactions to have a reliable study. In order to study a single compound, you need to reduce the variables. Could the statin drugs inhibit the effects of niacin? We may never know. In conclusion why have them on the least effective, most dangerous forms of niacin available? Why use laropiprant to prevent the niacin flush? Why select people who are on statins? So you can have the headlines that say niacin is harmful -- maybe? Moving on to the benefits. One of the noted benefits is the anti-inflammatory effect on arthritis. In an excellent article, "Several researchers have reported excellent results in arthritic patients using niacinamide. While niacin opens up the blood vessels near the surface and causes a flushing sensation, niacinamide only opens up the deep blood vessels like those surrounding the joints. In cases of moderate arthritis, outstanding results have been produced by taking 1,000 to 1,500 mg a day. In more severe cases, as much as 3,000 mg to 4,000 mg have been recommended." For dealing with cholesterol, it raises the production of HDL and reduces triglycerides and LDL. The article continues, "One of the most effective and least expensive ways to lower blood lipids (cholesterol and triglycerides) is to take 1,000 to 3,000 mg of niacin a day. Patients using 1,000 mg the first day, 2,000 mg the second day, and 3,000 mg each day thereafter have seen as much as a 25 percent reduction in cholesterol levels, and a 50 percent reduction in triglycerides. (Blood lipid reduction is the case where niacinamide is not as effective as niacin.)" Another reference manual from Berkley Heart Labs concluded their study of Lp(a) (the lipoprotein(a) is one of the most dangerous blood markers for CHD) "Treatments for elevated Lp(a) levels have variably reported analyte-lowering benefits. Lifestyle modifications such as diet, weight loss, and exercise generally have little or no effect on Lp(a) levels. Compared to the well reported LDL-lowering effects of statins and bile acid sequestrants (resins), these drugs generally also have little, or no effect on Lp(a) levels. Based on the best available study data, Niacin is the most effective drug option to treat Lp(a) elevations." This study in 2002 was conclusive though some, 21%, did not like the regimen due to the flushing response. Though it lowered their Lp(a) and improved their other lipid profiles, they did not stay with the treatment. It's been known to help with: Reversing heart disease Senility, memory loss, depression, insomnia Sun sensitivity Motion sickness Tinnitus, vertigo or hearing problems Improved circulation in legs of diabetics Migraine headaches It's not a perfect vitamin. You need to be aware that there are side effects like irritated stomach lining or ulcers and gout flare-ups. Be sure to take niacin on a full stomach, right after a meal is best. Several sources recommend consulting your doctor prior to taking niacin, especially in high doses. We've been taking straight niacin, 500mg as pictured above. My first dose which was about 1 hour after a meal, caused quite the rush of blood to the surface of my skin, it felt like a sunburn all over my face, neck and abdomen. It lasted about an hour and then subsided. Then the next morning dose I felt a small warming sensation, the evening dose had very little effect on me. Your body does adapt to the niacin once your levels come up. It takes about 2 days to reduce the effects, but they are not painful, some enjoy the warming feeling. This is my second blood test after starting the low-carb/high-fat (LCHF) lifestyle over 2 years ago. In the past 3+ months, we've gone into ketosis. These numbers are pretty good, but I'll explain why in a minute. The first test (pictured below) is the Atherotech VAP, which is an actual particle count, vs. the estimated LDL formula on a typical lipid panel. In case you did not know, the LDL is estimated using a formula created in 1974, so we're generally depending on a formula to estimate the "bad" cholesterol instead of measuring it directly. I chose this test in addition to my normal tests after reading the books, "Don't Die Early" and "The Great Cholesterol Myth." This shows size and type of particles measured directly. It is much more useful information to know the size and density of the cholesterol in your bloodstream. It also measures the other critical components like triglycerides and Lp(a). For those with the gift of seeing the obvious, I have four results that show HIGH, so it must be alarming & bad, right? First, lets look at the good & great stuff. My HDL (good) is 94 which is 19 points higher than last time. Any number higher than 45 in men is good; I'm more than double. My triglycerides are 48, which is very low, considering 150 is the level which causes concern; I'm less than 1/3 threshold. That low number is most likely due to my no-sugar, no-wheat, no-corn diet. But wait, I thought eating all that saturated fat makes a whole bunch of fat show up in your blood, right? Not if you're a fat-burning machine -- it gets consumed. Fat is dangerous when it is combined with wheat and sugars. (can you say doughnut?) because you're burning glucose, the fat is still floating around in your blood, then the sugar and wheat inflames your arteries creating lesions where the small dense LDL particles can lodge and start to build up into plaque. So the total cholesterol of 233 is high, right? Well, people with cholesterol of 250 have heart attacks and so do people with 150. There is no direct correlation between high cholesterol and heart disease, in fact there is no correlation between high LDL and heart disease. A recent study of almost 140,000 patients admitted to the hospital for heart disease, almost half of them had LDL levels under 100 mg/dL. So the Lipoprotein(a) is the more serious one because that is the one that is sticky and collects on the arterial walls and promotes cardiac plaque. The issue is the definition of HIGH. Upon reading these results, I was a little scared that I was at 17 and the baseline is at 10. According to two sources, 30 mg/dL is considered elevated and one source said 20 mg/dL is to top of the normal range. Source 1 Track Your Plaque site and Source 2 NIH.gov. A quote from the prolipid.com site states this, "You may notice Lipoprotein(a) or Lp(a) on your medical chart. Lp(a) is a subtype of LDL, and individuals with high levels of Lp(a) or "very bad" LDL, appear to be at higher risk for heart disease. Researchers can't seem to agree on the exact level of "high" Lp(a), but most specialists consider a value of approximately 30 mg/dL (0.8 mmol/l) to be high." The VLDL at 13, and VLDL-3 being low is encouraging. These are the small, sticky guys who cause problems with your arteries. The good news is, a simple solution for lowering my LDL is available. It's Niacin, or vitamin B3. 500mg per day, some sources up to 3g, are recommended to lower Lp(a) up to 20-30%. I may choose to increase my niacin and see what that does to my numbers next year. More to come, next week I'll be getting my physical with more numbers...stay tuned. 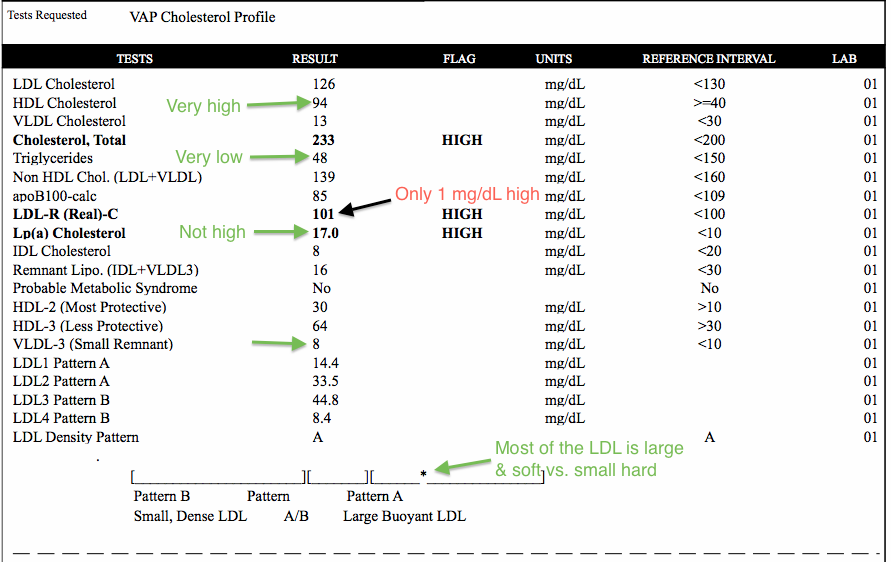  Finally some news that is worth reading. The LA Times just ran a story on Oct 22nd 2013 "Time to end the war against saturated fat?" It was refreshing to know that I was not the only one talking about the benefits of a low-carb/high-fat diet. "British Medical Journal has issued a clarion call to all who want to ward off heart disease: Forget the statins and bring back the bacon (or at least the full-fat yogurt). Saturated fat is not the widow-maker it's been made out to be, writes British cardiologist Aseem Malhotra" The story's lead paragraph read. Ahhh, bacon! Though the LA Times is for readers who don't generally want too much science, it was rooted in a solid peer reviewed BMJ article with some provoking questions entitled "Saturated fat is not the major issue" by Dr. Aseem Malhotra, interventional cardiology specialist registrar, Croydon University Hospital, London, brought up the fact that shortly after the US stated that saturated fat was deadly, studies were already disproving the heralded "seven countries" study. Which concluded "that a correlation existed between the incidence of coronary heart disease and total cholesterol concentrations, which then correlated with the proportion of energy provided by saturated fat. But correlation is not causation. Nevertheless, we were advised to cut fat intake to 30% of total energy and saturated fat to 10%.” (1) "The aspect of dietary saturated fat that is believed to have the greatest influence on cardiovascular risk is elevated concentrations of low density lipoprotein (LDL) cholesterol. Yet the reduction in LDL cholesterol from reducing saturated fat intake seems to be specific to large, buoyant (type A) LDL particles, when in fact it is the small, dense (type B) particles (responsive to carbohydrate intake) that are implicated in cardiovascular disease" (2) To summarize, carbs create small dense LDL particles which are bad news, but saturated fats are large and very large LDL particles which are harmless. What about cholesterol? The first response I get when I tell people that a high-fat diet is great for weight loss and energy, they say something about cholesterol. "I have high cholesterol, I can't do a high-fat diet" or something along that line. Well, good news! (not really new news) but the correlation of cholesterol and heart disease has not been proven. "Despite the common belief that high cholesterol is a significant risk factor for coronary artery disease, several independent population studies in healthy adults have shown that low total cholesterol is associated with cardiovascular and non-cardiac mortality, indicating that high total cholesterol is not a risk factor in a healthy population." (3), (4), (5) Notice the dates, 1994, 2002, some of these studies have been out there for a long time, peer reviewed and published, how come they have not hit the mainstream medical community? Is it that "the science is settled" argument and we move on with our blinders on? I hope not! Aseem Malhotra states "A recent “real world” study of 150 000 patients who were taking statins showed “unacceptable” side effects—including myalgia, gastrointestinal upset, sleep and memory disturbance, and erectile dysfunction—in 20% of participants, resulting in discontinuation of the drug.(6) This is massively at odds with the major statin trials that report significant side effects of myopathy or muscle pain in only one in 10 000." Statin drugs are a huge business. Pfizer’s Lipitor was the world’s top-selling medicine in 2010, according to IMS, raking in sales of $13.3billion. AstraZeneca’s Crestor, which garnered $5.38billion in sales during 2009, is one of the company’s best selling medicines. Total sales last year of cholesterol-treating medicines - including statins - were $35billion, according to IMS. So if you follow the money, it's a tough decision to state publicly that it's not really necessary to take statin drugs to lower cholesterol when you can reduce your carb intake and get the same results. From a UK Telegraph article "Despite the commercial success of statins, Dr Mali, (a pharmaceuticals analyst at Matrix Partners), out that the persistence of heart disease does raise questions about the drugs’ value for money. “Statins have been the fairy tale story in the industry. But heart disease is still the number one killer in the western world, so one could argue how much value for money have we really got out of their use,” he said." Aseem Malhotra stated a stinging truth "Adopting a Mediterranean diet after a heart attack is almost three times as powerful in reducing mortality as taking a statin. The recently published PREDIMED randomised controlled trial was stopped early after it showed that in high risk people the Mediterranean diet achieved a 30% improvement over a “low fat” diet in terms of cardiovascular events.(7) Dr, Malhotra states finally "It is time to bust the myth of the role of saturated fat in heart disease and wind back the harms of dietary advice that has contributed to obesity." So if I were reading this correctly, saturated fat, in his professional opinion, is not the culprit, but the dietary advice that has been given since Ancel Keys somehow won over the hearts and minds of the world in the 1970's; that is the problem. A low fat diet makes you fat & sick, while a low carb/high fat diet makes you skinny. Pass the bacon! (Organic of course) Footnotes
1. Committee on Medical Aspects of Food Policy. Diet and cardiovascular disease: report of the panel on diet in relation to cardiovascular disease. 1984 2. Musunuru K. Atherogenic dyslipidaemia: cardiovascular risk and dietary intervention. Lipids2010;45:907-14.CrossRef, MedLine 3. Nago N, Ishikawa S, Goto T, Kayaba K. Low cholesterol is associated with mortality from stroke, heart disease, and cancer: the Jichi Medical School Cohort Study. J Epidemiol2011;21:67-74.CrossRef Medline 4. Bae J-M, Yang Y-J, Li Z-M, Ahn Y-O. Low cholesterol is associated with mortality from cardiovascular diseases: a dynamic cohort study in Korean adults. J Korean Med Sci2002;27;58-63. 5. Simes RJ. Low cholesterol and risk of non-coronary mortality. Aust N Z J Med1994;24:113-9.Medline 6. Zhang H, Plutzky J, Skentzos S, Morrison F, Mar P, Shubina M, et al. Discontinuation of statins in routine care settings. Ann Intern Med2013;158:526-34. MedLine 7. Estruch R, Ros E, Salas-Salvadó J, Covas MI, Corella D, Arós F, et al. Primary prevention of cardiovascular disease with a Mediterranean diet. N Engl J Med2013;368:1279-90. CrossRef MedLine Why are we dealing with so many illnesses? Why are people losing their gallbladders in their forties? Why is dementia and alzheimer's on the rise? What about the dramatic decrease in sperm count? How come so many people have vitamin D deficiency? With all of our technology, mapping the human genome and all, huge sums of money for research -- where are the answers? We'll be doing at least a four-part series on these topics. For more than the past 50 years, we've been told that we need to reduce our fats. Even today's American Heart Association continues this mantra: Limit foods and beverages high in calories but low in nutrients, and limit how much saturated fat, trans fat, cholesterol and sodium. Read labels carefully — the Nutrition Facts panel will tell you how much of those nutrients each food or beverage contains. So, since we seem to always question the status quo, (because it's not working) let's look into this from the position of evidence and facts. Perhaps we'll discover the answers together. Gallbladders First you need a little Anatomy-Physiology 101 I mentioned in my WHY the challenges of being a teacher with all the constant goodies that are always left for anyone in the break room. I am a high school Chemistry, Biology and Anatomy Teacher. This write up will feature the scoop on the way our livers and gallbladders interact with the foods we eat, in a simple and generalized way so it is easy to understand the basics. Our livers are responsible for cleaning toxins out of our blood, making cholesterol (or transforming it into different types), getting rid of bilirubin (the remains of dead red blood cells), and supporting digestive processes. Toxins are released from the blood into the liver and end up in the bile ducts that feed into the gallbladder as the toxins drain from the ducts. Not every toxin travels this way, but many metabolic toxins do. When the day is done, up to 1,500 mL of bile has been produced. If the small intestines are empty, the gallbladder is in storage mode, holding all the bile to be released once food comes along. When food comes through the intestine, the duct will open from the gallbladder and bile will begin to drain. However, when fats or proteins come through the intestine it signals the release of cholecystokinin (CCK). This hormone causes the gallbladder to contract and empty its contents into the small intestine and stimulates the release of pancreatic juices to also be released. The more times the gallbladder empties, the more bile will flow out of the gallbladder and out of the liver. When the gallbladder doesn’t contract regularly the bile salts irritate the lining of the gallbladder so that the bladder produces mucus that causes a thickening of the bile contents. Continued storage of this substance causes the formation of stones -- gallstones. Since toxins are released from the body through the liver/bile processes, it stands to be smart to make sure the gallbladder receives the signal for full release of the gallbladder contents frequently to keep the liver and gallbladder clean. America has been experiencing epidemic levels of gallstones followed by gallbladder removal surgeries. Another issue of note is the frequency needed for the cleansing of the liver using herbal remedies, that is being touted by the alternative health community for the past 15-20 years. It is interesting to consider the drop in the consumption of animal fats and the rise of liver and gall bladder issues; could there be a connection? I realize that many reading this may no longer have their gallbladders, but the gall is still flowing from your liver. You should still be able to enjoy living on this food plan if you space out your fat consumption and figure out your rhythm of when your body does better with the fat, as in finding when your body is releasing more bile. I am aware of the pain and discomfort that can come from the lack of bile. Choosing which fats is also key. In conclusion, keeping your liver clean and your gallbladder healthy takes fats, lots of fats and good protein. If you are interested in cleansing your liver, even if you have had your gallbladder out, here’s a terrific resource that has proven effective for us and family members that have used it. The Liver and GallBladder Miracle Cleanse by Andreas Moritz, Ulysses Press, 2007 Cheers to a healthy liver! Lynette On the Atkins site, this article addresses things directly and is well cited: "In recent years surgeons have been increasingly removing gallbladders, presumably in an attempt to treat gallstones and related disorders. But the gallbladder is fundamental to your well-being. Among other functions, it stores bile, a powerful fat-emulsifying substance that the liver makes from cholesterol. A healthy gallbladder works with flawless precision, releasing bile just when it’s needed to help digest food. It also absorbs nutrients and keeps your cholesterol levels in check. Even as many doctors subscribe to the myth that eating fat and cholesterol leads to gallstones, research indicates that eating too little fat and too many carbohydrates in the form of grains, sugars and starches actually leads to gallbladder ailments."(1) One study did discover that low fat, high carb diets caused more gallstones than expected. "Conclusions: Our findings suggest that a high intake of carbohydrate, glycaemic load, and glycaemic index increases the risk of symptomatic gallstone disease in men. These results add to the concern that low fat high carbohydrate diets may not be an optimal dietary recommendation." Another study stated even more clearly: "In the obese during rapid weight loss from a very low calorie diet, a relatively high fat intake could prevent gallstone formation, probably by maintaining an adequate gallbladder emptying, which could counterbalance lithogenic mechanisms acting during weight loss." There were several studies that discussed the side-effect of gastric banding and the dramatic weight loss actually caused gallstones to develop in obese subjects. Dietary fat and cholesterol promote normal gallbladder function.(2) If you take cholesterol-lowering drugs, be aware that they can raise the risk of gallstone formation. Conclusion Consuming sufficient healthy fat (saturated & monounsaturated) while shunning sugar and other carbohydrates promotes gallbladder contractions and prevents gallstones better than anything else. So, long before surgery becomes a necessity, look at changing your diet. It’s a lot safer. For those of you who have lost your gallbladder, you can still eat a low carb/high fat diet. Footnotes
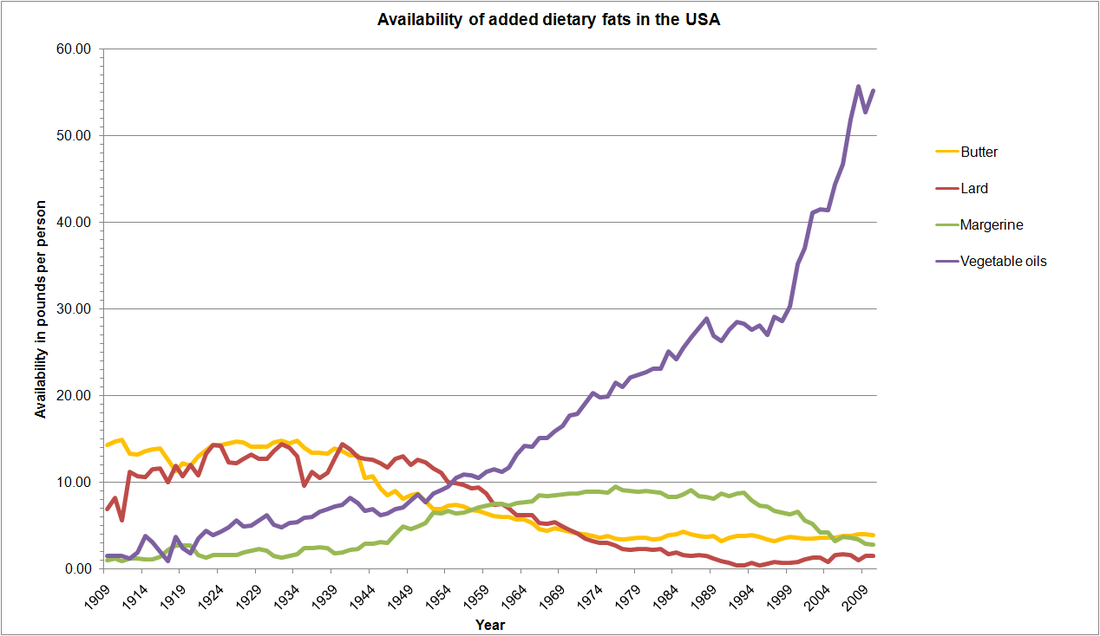
1. Tseng, M., Everhart, J.E., Sandler, R.S., "Dietary Intake and Gallbladder Disease: A Review," Public Health Nutrition, 2(2), 1999, pages 161-172. 2. Gebhard, R.L., Prigge, W.F., Ansel, H.J., et al., "The Role of Gallbladder Emptying in Gallstone Formation During Diet-Induced Rapid Weight Loss," Hepatology, 24(3), 1996, pages 544-548.3. Michielsen P.P., Fierens, H., Van Maercke, Y.M., "Drug-Induced Gallbladder Disease. Incidence, Aetiology and Management," Drug Safety, 7(1), 1992, pages 32-45.  It's so common to show greasy foods like french fries, hamburgers and show how fatty it is. Yes they are bad for you, but it's the inflammation caused from the vegetable oil or the hamburger bun, not the fatty burger that is bad for you. So if you've read my story, you know that I eat a lot of fat. 70-75% of my 2000 calories per day diet comes from fat. When I say that, most people say, "good fats, right?" I say, "Yeah good like bacon fat, saturated fat, coconut oils." Most people make a classic 'disgust' face when I say saturated fats. When I say organic & grass-fed, they seem to warm up to the idea. Then they are very confused that eating fats could be good for them. Eating this way has reduced my triglycerides, increased my HDL and reduced my blood pressure. If this experiment of N=1 were the only one it would be interesting, but there are so many with similar stories. In fact it seems that is the way it works, you reduce your carbs, replace those calories with fats and your body springs back into health. It is a complex balance of Omega 3/6 fats that reduces inflammation and turns you into a fat-burning machine that gives you the results. But as you can see, you'll be swimming upstream if you try this lifestyle. Like we've said, sugar is everywhere, so are inflammatory oils. So what happened to our diets in the past century that caused all this disease? We reduced our animal fats for sure, however we increased our vegetable oils. The problem with vegetable oils they are very high in Omega 6 fatty acids. Vegetable oil consumption rose dramatically between the beginning and end of the 20th century, and this had an entirely predictable effect on the ratio of omega-6 to omega-3 fats in the American diet. Between 1935 and 1939, the ratio of n-6 to n-3 fatty acids was reported to be 8.4:1. From 1935 to 1985, this ratio increased to 10.3:1 (a 23% increase). Other calculations put the ratio as high as 12.4:1 in 1985. Today, estimates of the ratio range from an average of 10:1 to 20:1, with a ratio as high as 25:1 in some individuals. In fact, Americans now get almost 20% of their calories from a single food source – soybean oil – with almost 9% of all calories from the omega-6 fat linoleic acid (LA) alone! (source) 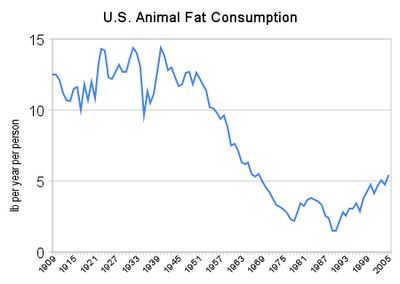
|
AuthorsTim & Lynette Jenné are learners first and foremost. We love to ask "why?" We question the status quo. We also love to research and find answers for ourselves. As parents of four adult children, we've learned a few things along the way that may be helpful to others. We love to live & eat clean, simple lives. Archives
July 2015
Categories |
 RSS Feed
RSS Feed